
Individuals living with Sickle Cell Disease (SCD) most often endure not only excruciating pain but also a multitude of emotional and physical challenges (Elendu et al., 2023; CDC). The unpredictable nature of the disease, along with its significant emotional and physical toll, drives those affected to seek out various coping mechanisms, with alcohol consumption often emerging as a notable choice. Despite the life-threatening nature of SCD, a substantial number of individuals with this condition engage in alcohol consumption, with approximately 32% of SCD patients turning to drink (Levenson et al., 2009). The perplexing question that arises is: What motivates these individuals to resort to alcohol despite the evident risks associated with such a choice?
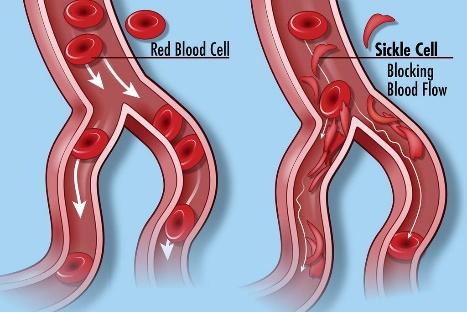
The persistent chronic pain associated with Sickle Cell Disease (SCD) serves as a primary catalyst for alcohol consumption among those affected. Sickle cell crises, characterized by intense and recurring pain episodes, pose a substantial challenge in identifying effective pain management strategies beyond prescribed medications. In such circumstances, alcohol, recognized for its analgesic properties, becomes an appealing option for individuals seeking relief from enduring discomfort (Thompson et al., 2017; Neddenriep et al., 2019). However, the unintended consequence emerges when individuals, in their attempt to alleviate pain through alcohol’s analgesic properties, may find themselves inadvertently entangled in a cycle of dependence. The initial pursuit of comfort through alcohol’s short-term relief can lead to a dependency that proves challenging to break free from. Over the long term or with chronic use, alcohol may have adverse consequences, potentially exacerbating the progression of chronic pain (Neddenriep et al., 2019; Woodrow & Eltherington, 1988; James et al., 1978; Blanton et al., 2019).

Living with sickle cell disease (SCD) exerts a significant emotional toll, and its profound impact should not be overlooked. The unpredictability of the disease, coupled with its physical challenges, can evoke feelings of isolation, anxiety, and despair. Psychological complications linked to SCD may manifest in various ways, including inappropriate pain coping strategies, diminished quality of life due to restrictions in daily functioning, and experiences of anxiety, depression, and neurocognitive impairment (Anie, K. A. 2005). The enduring presence of pain can further amplify this emotional burden, fostering a sense of hopelessness and helplessness, and potentially contributing to the onset of depressive symptoms (Al-Dewik & Ghebremeskel, 2014). Faced with these challenges, some individuals may turn to alcohol as both a coping mechanism and a temporary means of escaping the emotional burdens imposed by SCD.
Managing chronic pain in individuals with Sickle Cell Disease (SCD) involves a reliance on high-dose opioids, increasing the risk of opioid dependency. The challenges in addressing persistent pain are compounded by the potential for opioid abuse, prompting certain SCD patients to seek alternative coping mechanisms. Racial bias within healthcare further complicates this pursuit, where care providers may perceive SCD individuals as challenging or unfairly label them as pretentious patients (Bergman & Diamond, 2013). This misinterpretation, coupled with possible restrictions on opioid prescriptions, leads to inadequate pain relief. The confluence of these challenges, along with the complexities of frequent hospital visits and unpredictable pain crises, further heightens the risk of social isolation for individuals with SCD, worsening feelings of depression (Edwards et al., 2008). Faced with this intricate web of difficulties, some individuals with SCD may turn to alcohol as an alternative coping strategy to seek relief from the chronic pain they endure amid limited pain management options and racial bias within the healthcare system.
The stigma surrounding chronic illnesses, such as sickle cell disease (SCD), can be isolating and emotionally burdensome. Stigma and discrimination further compound the struggles of those with SCA. Individuals may encounter discrimination or stigmatization based on misunderstandings about the condition, resulting in diminished self-esteem and the onset of depressive symptoms (Treadwell, Telfair, & Gibson, 2008). Grappling with societal misconceptions and a lack of understanding about their condition, some individuals may resort to alcohol as a coping mechanism, seeking a perceived sanctuary from these challenges. Considering these difficulties, there is a pressing need for increased awareness and sensitization about SCD in society. Education and understanding can help dispel misconceptions, reduce stigma, and create a more supportive environment for individuals with SCD. Additionally, family members play a crucial role in providing support and understanding, emphasizing the importance of rallying familial support networks to better assist those affected by SCD in navigating the challenges they face.

Access to comprehensive healthcare is crucial for effectively managing Sickle Cell Disease (SCD). Unfortunately, economic hardships often create barriers for many individuals with SCD to obtain the necessary medical resources. Financial constraints, coupled with inadequate health insurance, make it challenging for these individuals to maintain consistent income—a struggle further intensified by the difficulties of securing stable employment due to the demands of their condition. This is especially apparent given that statistics reveal approximately 70% of individuals of working age with Sickle Cell Disease are not engaged in employment, indicating a profound adverse effect on their job prospects. As a result, there is a high social cost represented by a very low monthly per capita income in 93.7% of these individuals (Pires et al., 2022). Moreover, it is estimated that patients with SCD lose around $700,000 over their lifetime because of their inability to work (Inserro, 2022). In real-life terms, the economic impact of SCD is substantial, with estimated costs reaching $1.6 million to $1.7 million throughout individuals’ non-elderly lives (0-64 years. For females with SCD, out-of-pocket (OOP) costs are estimated at $42,395, while for males, the corresponding estimate is $45,091. Compared to individuals without SCD, this represents a staggering 907% increase in total medical costs and a 285% increase in OOP costs. While this is based on the commercially insured population, it emphasizes the significant financial burden of SCD (Johnson et al., 2023)
The convergence of economic challenges, lack of insurance, and unemployment compounds the struggle for most individuals with SCD, potentially driving them to resort to alcohol as a means of self-medication. This coping strategy may be particularly prevalent among those lacking insurance and grappling with unemployment, introducing an additional layer of complexity to the myriad challenges faced by these individuals in managing both the physical and emotional aspects of SCD.
In summary, the complex interplay of factors surrounding Sickle Cell Disease, including the reliance on opioids, racial bias, societal stigma, economic hardships, and the allure of alcohol as a coping strategy, underscores the need for an all-rounded approach. Addressing these challenges requires a comprehensive strategy that includes improving healthcare access, providing economic support, and combatting societal stigma. Educating healthcare providers to ensure unbiased care, exploring alternative pain management, and offering essential mental health support are crucial elements. Additionally, enhancing easier access to employment opportunities and advocating for insurance reforms contribute to a supportive environment. This comprehensive strategy aims to improve the overall quality of life for individuals navigating the complexities of SCD.