The quest for effective management of chronic pain in Sickle Cell Disease (SCD) has seen little progress, despite the emergence of new drugs aiming to mitigate the frequency of the disease’s crises. Current treatments fall short of addressing the chronic pain that 54% of individuals with SCD endure for more than half of their lives (Smith et al., 2008). With most patients managing their pain at home, the severity of their suffering is often underestimated by healthcare providers, leading to a treatment gap. Against this backdrop, cannabis—also known as marijuana, pot, or Mary Jane—emerges as an innovative approach that is utilized by some of the individuals grappling with Sickle Cell Disease to alleviate the severity of their painful episodes. Crucially, over 33% of adults with sickle cell disease (SCD) admit to using cannabis-based products (Curtis et al., 2020). However, the pressing question remains: Is it safe?

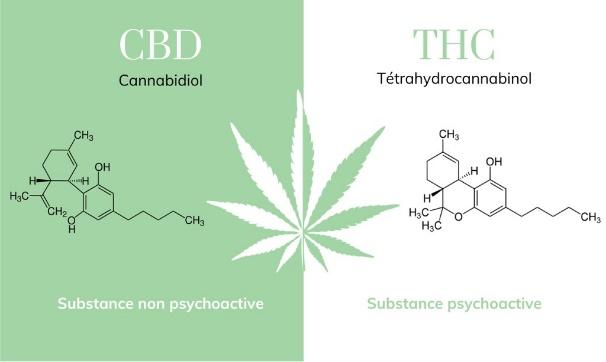
Marijuana contains a wealth of cannabinoids, including tetrahydrocannabinol (THC) and cannabidiol (CBD), which show remarkable potential in pain management, particularly for those grappling with Sickle Cell Disease. THC, the main psychoactive element in marijuana, stimulates the release of dopamine, a neurotransmitter linked to pleasure, in the brain (Bloomfield et al., 2016; Bossong et al., 2009; Oleson and Cheer, 2012). This process leads to a euphoric state commonly referred to as feeling ‘high,’ thereby affecting mood and the sense of reward (Cafasso, 2022; Abrams et al., 2020; Healthline blog). Moreover, both THC and CBD interact with the CB-1 and CB-2 receptors in the immune and central nervous systems. These interactions are crucial in moderating pain and inflammation, particularly in SCD, where they represent the primary symptoms.
Smoking is the most preferred form of cannabis administration (Curtis et al., 2020). However, for individuals with Sickle Cell Disease (SCD) who may already be facing respiratory challenges, including Acute Chest Syndrome, this practice could further aggravate their condition. This calls for the urgent need for further research to determine if alternative methods of administration, such as cannabis extracts, might be more effective and safer in managing pain for those with Sickle Cell Disease.
Despite the potential benefits that cannabis has shown in managing SCD, a research team from the University of Michigan Medical School and the VA Ann Arbor Healthcare System found that over 50% of individuals who use medical marijuana products for pain relief experience clusters of multiple withdrawal symptoms during periods between uses. The study further revealed that marijuana contributes to deteriorating changes in sleep, mood, mental state, energy, and appetite. Of utmost concern is that the withdrawal symptoms do not directly stem from the individuals’ underlying conditions but rather from the brain and the body’s response to the absence of active ingredients in the cannabis introduced into the body.
Cannabis withdrawal syndrome manifests when individuals experience symptoms such as heightened anxiety, disrupted sleep patterns, diminished appetite, restlessness, a sense of depression, and increased aggression. If these symptoms are severe, they can potentially metamorphize into Cannabis Use Disorder. This arises when individuals attempting to reduce or quit cannabis face intensified symptoms, making it difficult to break free from the cycle. Ultimately, this heightened severity can lead individuals to misinterpret the symptoms and associate them with their medical conditions. Consequently, it sets off a challenging cycle of increased cannabis use that is hard to break.
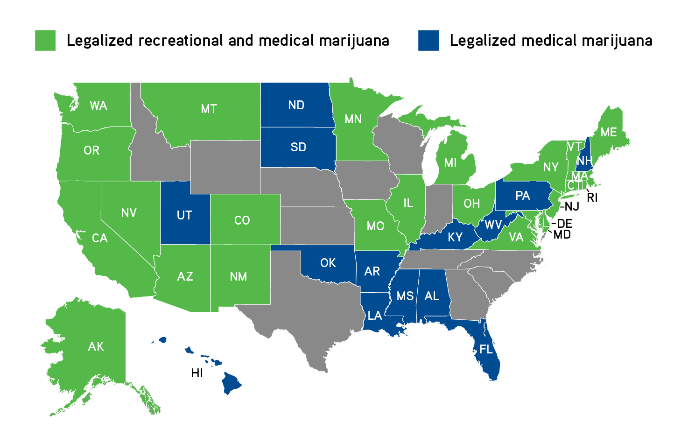
According to ProCon.org, as of June 2022, 37 states along with the District of Columbia have legalized the use of marijuana for qualifying medical conditions, marking a steady increase in the accessibility of medical marijuana across the United States. However, it’s important to highlight that among these, only nine states acknowledge sickle cell disease (SCD) as a condition eligible for medical marijuana treatment. Despite this growing acceptance, the Food and Drug Administration (FDA) has yet to approve any cannabis products specifically for the treatment of pain related to SCD. The FDA has approved cannabinoids, such as Epidiolex (which contains CBD), exclusively for treating two rare forms of epilepsy (Cafasso, 2022, Healthline blog). As a result, individuals with SCD seeking pain relief may face potential risks when resorting to marijuana products sourced from unofficial channels. The situation is further complicated by the fact that adults with Sickle Cell Disease (SCD) often turn to cannabis due to receiving insufficient opioid dosages from their medical caregivers. Additionally, they face increased stigmatization when seeking higher doses of these analgesics, coupled with a lack of alternative options for pain relief (Sinha et al., 2019; Argueta et al., 2020).
The management of pain associated with Sickle Cell Disease presents a significant challenge within the medical community, with cannabis emerging as a prospective yet intricate solution. Although numerous studies have indicated favorable outcomes, the presence of contradictory results alongside the absence of formal approval by the Food and Drug Administration (FDA) accentuates the imperative for further extensive research into the effectiveness and safety of cannabis for pain relief in SCD. Furthermore, the necessity to achieve a delicate balance between efficacious pain management, enhancement of mood, and the mitigation of potential adverse effects underscores the critical importance of individualized medical decisions. This is particularly pertinent given the stigmatization and difficulties encountered by adults with SCD in the hands of their healthcare providers.